Succinylcholine Depolarizing Neuromuscular Blocker
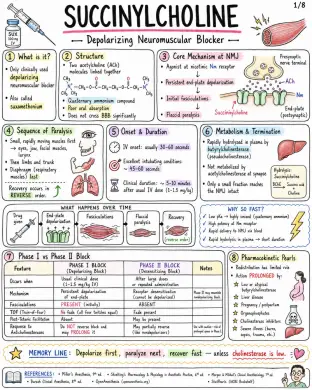
Image 1: What is it: - Only clinically used depolarizing neuromuscular blocker - Also called suxamethonium Structure: - Two acetylcholine (ACh) molecules linked together - Quaternary ammonium compound - Poor oral absorption - Does not cross BBB significantly Core Mechanism at NMJ: - Agonist at nicotinic Nm receptor - Persistent end-plate depolarization - Initial fasciculations - Flaccid paralysis Sequence of Paralysis: - Small, rapidly moving muscles first → eyes, jaw, facial muscles, larynx - Then limbs and trunk - Diaphragm (respiratory muscles) last - Recovery occurs in REVERSE order Onset & Duration: - IV onset: usually 30–60 seconds - Excellent intubating conditions: ~ 45–60 seconds - Clinical duration: ~ 5–10 minutes after usual IV dose (1–1.5 mg/kg) Metabolism & Termination: - Rapidly hydrolyzed in plasma by butyrylcholinesterase (pseudocholinesterase) - Not metabolized by acetylcholinesterase at synapse - Only a small fraction reaches the NMJ intact Phase I vs Phase II Block: - Phase I Block (Depolarizing Block): - Occurs when: Usual clinical dose (1–1.5 mg/kg IV) - Mechanism: Persistent depolarization of end-plate - Fasciculations: PRESENT (initially) - TOF (Train-of-Four): No fade (all four twitches equal) - Post-Tetanic Facilitation: Absent - Response to Anticholinesterases: Do NOT reverse block and may PROLONG it - Phase II Block (Desensitizing Block): - Occurs when: After large doses or repeated administration - Mechanism: Receptor desensitization (cannot be depolarized) - Fasciculations: ABSENT - TOF (Train-of-Four): Fade present - Post-Tetanic Facilitation: May be present - Response to Anticholinesterases: May partially reverse (like nondepolarizers) Pharmacokinetic Pearls: - Redistribution has limited role - Action PROLONGED by: - Low or atypical butyrylcholinesterase - Liver disease - Pregnancy / postpartum - Organophosphates - Cholinesterase inhibitors - Severe illness (burns, sepsis, trauma, etc.) WHY SO FAST? - Low pKa → highly ionized (quaternary ammonium) - High potency at Nm receptor - Rapid delivery to NMJ via blood - Rapid hydrolysis in plasma → short duration Image 2: Main Indications: - Rapid sequence intubation (RSI) - Emergency airway control - Brief procedures requiring intense, short paralysis - Treatment of laryngospasm (small dose IV in selected settings) - Facilitation of electroconvulsive therapy (ECT) Standard Dosing: - Route: IV (intubation dose), ED/RSI (commonly IV), IM (when IV unavailable) - Dose: 1-1.5 mg/kg, 1-1.5 mg/kg, 3-4 mg/kg (max practical dose ~150 mg) - Onset: 30-60 seconds, 30-60 seconds, 2-3 minutes - Duration: ~5-10 minutes, ~5-10 minutes, Longer than IV (typically 15-20+ min) Why Favored for RSI: - Fastest onset of all neuromuscular blockers - Profound, reliable muscle relaxation - Short duration → quick recovery of spontaneous breathing - Excellent intubating conditions Succinylcholine vs. Rocuronium for RSI: - Feature: Typical RSI dose, Onset (IV), Duration, Reversibility, Major Advantages, Major Disadvantages - Succinylcholine: 1-1.5 mg/kg IV, 30-60 seconds, ~5-10 minutes, Spontaneous (no specific reversal agent), Fastest onset, ultra-short duration, excellent conditions, Hyperkalemia risk, MH risk, apnea, other adverse effects - Rocuronium: 1.0-1.2 mg/kg IV, ~45-60 seconds, ~30-60 minutes, Reversible with sugammadex, No risk of malignant hyperthermia or hyperkalemia, Longer duration unless reversed; slightly slower onset Dosing Pearls: - Weight to use: Many clinicians dose SUX to TOTAL BODY WEIGHT (TBW) in obesity because of increased pseudocholinesterase activity and larger extracellular fluid volume - Reduced dose 0.3-0.6 mg/kg may relieve laryngospasm, but may be inadequate for full intubating paralysis - Defasciculation: Give a small dose of a nondepolarizing neuromuscular blocker (e.g., rocuronium 0.1 mg/kg IV) 1-3 min before SUX to reduce fasciculations and myalgia. May slightly increase SUX intubating dose requirement Sequence of Clinical Onset (IV): - Jaw relaxation: ~30–45 sec - Cords open: ~45–60 sec - Apnea & paralysis: ~60 sec - Recovery: ~5–10 min Monitoring & Administration Reminders: - Use ONLY when airway equipment and ventilation capability are immediately available - Always give with adequate sedation or anesthesia and analgesia - Preoxygenate before administration - Confirm IV access and patency, Monitor clinical effect closely - Neuromuscular monitoring (TOF, PTC, or acceleromyography) recommended Image 3: Fasciculations: - Mechanism: brief depolarization of muscle end-plates → synchronous muscle twitches - Common after administration (almost universal) - May cause postoperative myalgia - More common in ambulatory patients / adults - Reduced by: Defasciculation (small dose nondepolarizing NMB), Lidocaine (IV 1-1.5 mg/kg), NSAIDs (e.g., ketorolac, ibuprofen) Myalgia: - Incidence variable (~10-50%) - Mechanism (theory): Muscle microtrauma from intense fasciculations → increased CK, muscle soreness - Typically affects masseter, neck, back, and extremities - Usually mild, self-limited (24-48 h) - More common in ambulatory patients and adults Bradycardia & Rhythm Effects: - Due to stimulation of cardiac muscarinic receptors (vagal effect) - More likely with: repeated doses, children, and conditions with high vagal tone - Dysrhythmias may occur (PVCs, junctional rhythm, asystole) - Atropine pretreatment (0.01-0.02 mg/kg IV) sometimes considered in pediatrics or with repeated dosing Increased Intraocular Pressure: - Transient rise begins within minutes after administration; resolves in 5-10 minutes - Due to contraction of extraocular muscles and decreased outflow - Historically relevant in open globe injury debate - Clinical decision individualized (benefits vs. risks) - Open globe injury? → Consider alternative NMB or risk mitigation Increased Intragastric & Intracranial Pressure: - Transient increase after administration - Offset by increased tone of lower esophageal sphincter - ICP increase is usually small and transient - Consider clinical context: TBI, space-occupying lesions, or uncontrolled ICP Histamine Release / Anaphylaxis: - Histamine release is generally minimal compared with some other agents - May cause flushing, hypotension, bronchospasm (rare) - Anaphylaxis can occur — as with all neuromuscular blockers Mechanism Map: From Depolarization to Effects: - Succinylcholine → Persistent depolarization at NMJ → Synchronous muscle firing → Fasciculations → Efflux of K+ → Serum potassium ↑ → Muscle fiber stress / microtrauma → Myalgia → Vagal stimulation (cardiac M2) → Bradycardia / Dysrhythmias Practical Management Pearls: - Ensure adequate depth of anesthesia before giving drug to blunt sympathetic responses. - Anticipate fasciculations — consider defasciculation or adjuncts. - Monitor ECG and hemodynamics; be prepared for bradycardia. - Be ready to ventilate and support blood pressure. - Avoid repeated doses when possible. Image 4: Hyperkalemia - Normal serum K+ rise ~ 0.5 mEq/L in healthy patients - Mechanism: Sustained depolarization → K+ efflux from muscle Dangerous Hyperkalemia Risk States - Burns after ~24-48 h and for months - Major denervation / spinal cord injury / stroke after ~24-72 h and may persist months - Prolonged immobilization / critical illness myopathy - Upper or lower motor neuron lesions - Muscular dystrophies / myopathies (especially Duchenne / Becker) - Severe infection or trauma with receptor upregulation - Rhabdomyolysis risk Malignant Hyperthermia Trigger - Succinylcholine can trigger MALIGNANT HYPERTHERMIA – especially with volatile anesthetics. - Early Signs: Rising ETCO2, Tachycardia, Muscle rigidity, Hyperthermia (later), Acidosis, Hyperkalemia - Management: - STOP triggers (SUX + volatiles) NOW - Call for HELP / activate MH protocol - Give DANTROLENE 2.5 mg/kg IV repeat as needed - Active cooling - Treat acidosis and hyperkalemia - Support ventilation and circulation Masseter Spasm / Jaw Rigidity - May occur with succinylcholine - Can be isolated but may herald MH - Do NOT assume it is a normal course Cardiac Arrest in Undiagnosed Myopathy in Children - Routine elective pediatric IM or IV use has become LIMITED because of rare but SEVERE hyperkalemic cardiac arrest in occult myopathy (e.g., Duchenne, Becker, other myopathies). - Use extreme caution. Emergency Algorithm - Suspect Complication (e.g., ↑ ETCO2, rigidity, arrhythmia, hyperkalemia) - Stop Drug Exposure / Trigger: Stop SUX and/or volatile anesthetics - Oxygenate / Ventilate: 100% O2 Ensure adequate ventilation - ECG / Electrolytes: Obtain 12-lead ECG Check K+, ABG, Ca2+, CK, etc. - Treat Specific Emergency: Treat hyperkalemia, treat MH, manage arrhythmias, support ACLS Memory Line: The big dangers are K+, MH, and occult myopathy. Act FAST. Delays can be FATAL. Image 5: Absolute / strong contraindications: - Personal or family history of malignant hyperthermia - Known pseudocholinesterase deficiency (butyrylcholinesterase deficiency) - Prior severe reaction / anaphylaxis to succinylcholine - Active hyperkalemia - Conditions with major extrajunctional receptor upregulation (↑ K+ risk): - Major burns after the first 24 h - Denervation injury (e.g., spinal cord injury) - Progressive neuromuscular disease (ALS, MS, muscular dystrophy) - Prolonged immobilization Use with major caution: - Open globe injury - Penetrating eye injury - Increased intracranial pressure risk (avoid large ↑ in ICP) - Severe sepsis / critical illness myopathy - Muscular dystrophy - Renal failure with pre-existing hyperkalemia - Recent stroke or spinal cord injury - Crush injury - Extensive trauma Special populations - key points: Population - Considerations - B