Midazolam
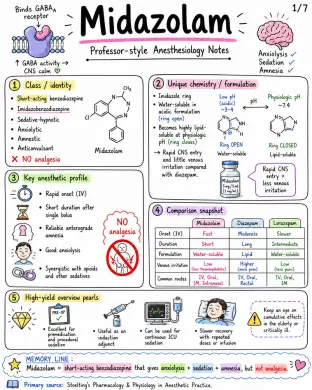
Handwritten notes about midazolam. Pharmcology, pharmacodynamics, pharmacokinetics, exam ready notes Image 1: Class / identity: - Short-acting benzodiazepine - Imidazobenzodiazepine - Sedative-hypnotic - Anxiolytic - Amnestic - Anticonvulsant - NO analgesia Unique chemistry / formulation: - Imidazole ring - Water-soluble in acidic formulation (ring open) - Becomes highly lipid-soluble at physiologic pH (ring closes) → Rapid CNS entry and little venous irritation compared with diazepam. Key anesthetic profile: - Rapid onset (IV) - Short duration after single bolus - Reliable anterograde amnesia - Good anxiolysis - Synergistic with opioids and other sedatives Comparison snapshot: - Onset (IV): Fast - Duration: Short - Formulation: Water-soluble - Venous irritation: Low (less thrombophlebitis) - Common routes: IV, Oral, IM, Intranasal High-yield overview pearls: - Excellent for premedication and procedural sedation - Useful as an induction adjunct - Can be used for continuous ICU sedation - Slower recovery with repeated doses or infusion - Keep an eye on cumulative effects in the elderly or critically ill. Image 2: Mechanism of action: - Positive allosteric modulator at GABA_A receptor - Increases frequency of chloride (Cl-) channel opening in the presence of GABA - More Cl- influx - Hyperpolarization - Neuronal inhibition CNS effects: - Sedation - Hypnosis - Anxiolysis - Anterograde amnesia - Anticonvulsant effect - Muscle relaxation - Decreases CMRO2, CBF, and ICP modestly → CPP usually preserved in many settings - EEG slows - No analgesia Respiratory effects: - Dose-dependent respiratory depression - Decreased ventilatory response to CO2 - Apnea possible after rapid IV bolus - Upper airway obstruction risk (especially in sedated/recumbent patients) - Effects are much greater with opioids, alcohol, propofol, or other sedatives Cardiovascular effects: - Mild-to-moderate decrease in SVR and BP - Small fall in cardiac output - Usually modest hemodynamic change in healthy patients - More hypotension in hypovolemia, elderly, or when combined with opioids/other anesthetics Other physiologic pearls: - Minimal histamine release - Little effect on neuromuscular transmission - May reduce recall strongly (anterograde amnesia) - Paradoxical agitation can rarely occur Image 3: Routes / absorption: - IV: 100% bioavailability, direct to circulation - IM: Reliable absorption, bioavailability ~90%+ - Oral: Incomplete bioavailability (~30–50%) due to first-pass metabolism - Intranasal: Useful in pediatrics and seizures - Buccal: Bypasses first-pass metabolism; alternative when IV not available Onset and duration: - IV (small bolus): Onset ~1–2 min, peak effect ~3–5 min, clinical duration ~20–30 min after small IV bolus - IM: Onset ~10–20 min - Oral: Onset ~15–30 min Distribution: - Highly lipophilic at physiologic pH - Rapid brain uptake - High protein binding (~95%) - Volume of distribution (Vd) increases in obesity Metabolism / elimination: - Metabolized by CYP3A4 to 1-hydroxymidazolam (active but weaker) - Elimination half-life (t½): ~1.5–3 hours in healthy adults - Glucuronidation (UGT enzymes) and renal excretion (urine) Context and special PK issues: - Effect is prolonged with repeated doses or infusions - Context-sensitive recovery increases as infusion duration increases - Special considerations: elderly, hepatic impairment, congestive heart failure, obesity, renal failure (metabolite accumulation) Image 4: Premedication: anxiolysis and amnesia before anesthesia - Adults (typical): - Oral: 7.5-15 mg - IM: ~0.07-0.1 mg/kg - IV: small titrated doses 0.5-2 mg - Pediatrics: - Oral: ~0.25-0.5 mg/kg (commonly max ~20 mg) - Intranasal: ~0.2-0.3 mg/kg Procedural sedation / monitored anesthesia care - IV titration in small increments - Often total 1-5 mg in healthy adults - Usually combined with analgesic (e.g., fentanyl) - Caution: respiratory depression Induction / co-induction - Induction dose if used alone: ~0.1-0.3 mg/kg IV - Lower doses as co-induction adjunct to reduce requirements of propofol or other anesthetics ICU / prolonged sedation - Intermittent bolus or infusion - Example: ~0.02-0.1 mg/kg/hr - Recovery may be delayed after long infusions Other important uses - Status epilepticus / seizure control (especially IV/IM/ intranasal) - Anxiolysis before regional anesthesia - Sedation in mechanically ventilated patients - Adjunct to reduce recall (amnesia) Always titrate to effect; reduce dose in elderly/frail patients. MEMORY LINE: Midazolam is most often used for premedication, procedural sedation, induction adjunct, and ICU sedation - always titrate carefully. Primary source: Stoelting's Pharmacology & Physiology in Anesthetic Practice. Image 5: Common adverse effects: - Excessive sedation - Drowsiness - Psychomotor impairment - Dizziness - Ataxia - Confusion - Postoperative delayed recovery Respiratory hazards: - Hypoventilation - Apnea - Airway obstruction - Especially after IV bolus or with opioids - Higher risk in OSA, COPD, obesity, elderly, and frail patients. Hemodynamic adverse effects: - Hypotension, especially in hypovolemia or with other anesthetics - Occasional bradycardia Neuropsychiatric issues: - Paradoxical agitation / disinhibition - Delirium in susceptible patients - Rare involuntary movements - Tolerance and withdrawal with prolonged ICU use Monitoring / practical safety: - Titrate slowly - Allow time between doses - Continuous pulse oximetry during sedation - Capnography when appropriate - Be prepared for airway support - Resuscitation drugs/equipment available Image 6: Major drug interactions: - CYP3A4 inhibitors → ↑ midazolam levels / ↑ effect - Erythromycin / clarithromycin - Azole antifungals (ketoconazole, itraconazole, voriconazole) - Protease inhibitors (e.g., ritonavir) - Diltiazem / verapamil - Grapefruit (juice) - CYP3A4 inducers → ↓ midazolam levels / ↓ effect - Rifampin, carbamazepine, phenytoin Marked synergistic respiratory depression with CNS depressants: - Opioids (e.g., fentanyl, morphine) - Propofol - Alcohol - Other sedatives / hypnotics (e.g., barbiturates, Z-drugs) Elderly / frail: - Increased sensitivity to midazolam - Smaller central volume of distribution - Reduced clearance → Start with much lower doses and titrate slowly Organ dysfunction: - Hepatic disease, heart failure, shock: Reduced clearance → prolonged effect - Renal failure: Active metabolite conjugates may accumulate, Prolonged sedation possible Special populations: - Obesity / OSA / pulmonary disease: Dose carefully, Higher risk of airway obstruction and delayed recovery - Pregnancy / neonates: Use only when clearly indicated, Neonatal respiratory depression and hypotonia can occur Contraindications / strong cautions: - Hypersensitivity to benzodiazepines - Severe respiratory compromise without ventilatory support - Acute narrow-angle glaucoma (classic benzodiazepine caution) - Myasthenia gravis / severe sleep apnea → use with caution - Midazolam alone DOES NOT provide analgesia for painful procedures. Image 7: Flumazenil Reversal: - Competitive benzodiazepine antagonist - Adult IV reversal commonly 0.2 mg increments titrated to effect (up to ~1 mg in many routine settings; higher cumulative doses possible) - Onset: rapid (1–2 min) - Duration shorter than some benzodiazepine effects → resedation can occur - CAUTION: May precipitate seizures in benzodiazepine-dependent patients or in mixed overdose with pro-convulsant drugs Midazolam vs Propofol: - Midazolam: Stronger amnesia, Slower recovery, No analgesia, Less hypotension in many patients, Reversible with flumazenil - Propofol: Less amnesia, Faster recovery, No analgesia, More hypotension, No reversal agent Midazolam vs Diazepam: - Midazolam: Water-soluble, Less venous irritation, Faster onset, Shorter recovery, More suitable for titrated IV sedation - Diazepam: Lipid-soluble, More venous irritation, Slower onset, Longer recovery, Less ideal for titrated IV sedation Professor Pearls / Viva Points: - No analgesia - Produces pronounced anterograde amnesia - Imidazole ring explains water solubility in vial - Metabolized in liver by CYP3A4 - Active metabolite (1-OH midazolam) can accumulate in renal failure - Combination with opioids greatly increases risk of apnea and respiratory depression - Flumazenil reverses, but watch for resedation Mini Algorithm / Checklist Before Giving Midazolam: 1. Assess airway & OSA risk - History - Airway exam - OSA / BMI 2. Consider age & comorbidities - Elderly - Hepatic / renal impairment - Cardiac disease 3. Check concurrent opioids / CNS depressants - Opioids - Alcohol / benzos - Other sedatives 4. Ensure IV access & monitoring - Pulse oximetry - BP / ECG - Capnography (if deep sedation) 5. Titrate slowly - Small IV doses - Titrate to effect - Pause and reassess 6. Observe recovery & discharge safety - Stable vitals - Alert / oriented - Escort / instructions