IV anesthesia induction agents
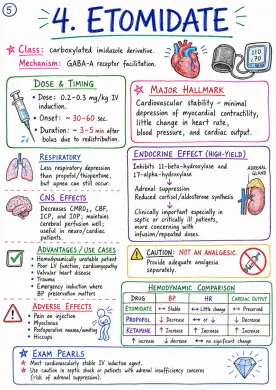
Image 1: Class: - carboxylated imidazole derivative Mechanism: - GABA-A receptor facilitation DOSE & TIMING - Dose: 0.2-0.3 mg/kg IV induction - Onset: ~ 30-60 sec - Duration: ~ 3-5 min after bolus due to redistribution MAJOR HALLMARK - Cardiovascular stability - minimal depression of myocardial contractility, little change in heart rate, blood pressure, and cardiac output RESPIRATORY - Less respiratory depression than propofol/thiopentone, but apnea can still occur ENDOCRINE EFFECT (HIGH-YIELD) - Inhibits 11-beta-hydroxylase and 17-alpha-hydroxylase - Adrenal suppression - Reduced cortisol/aldosterone synthesis - Clinically important especially in septic or critically ill patients, more concerning with infusion/repeated doses CNS EFFECTS - Decreases CMRO2, CBF, ICP, and IOP; maintains cerebral perfusion well; useful in neuro/cardiac patients ADVANTAGES / USE CASES - Hemodynamically unstable patient - Poor LV function, cardiomyopathy - Valvular heart disease - Trauma - Emergency induction where BP preservation matters ADVERSE EFFECTS - Pain on injection - Myoclonus - Postoperative nausea/vomiting - Hiccups CAUTION: NOT AN ANALGESIC - Provide adequate analgesia separately HEMODYNAMIC COMPARISON - DRUG: Etomidate, Propofol, Ketamine - BP: Stable, Decrease, Increase - HR: Little change, or ↓, Increase - CARDIAC OUTPUT: Preserved, Decrease, Increase EXAM PEARLS - Most cardiovascularly stable IV induction agent - Use caution in septic shock or patients with adrenal insufficiency concerns (risk of adrenal suppression) Image 2: Main Drug Focus: - Midazolam - Also: Diazepam, Lorazepam (Older/less common choices for induction) Mechanism: - Benzodiazepines enhance GABA-A receptor action by increasing the frequency of chloride channel opening. Midazolam - Key Properties: - Water soluble in acidic formulation; becomes lipid soluble at physiologic pH → rapid CNS entry Effects: - Anxiolysis - Sedation - Hypnosis - Anterograde amnesia - Anticonvulsant action - Muscle relaxation Doses (IV): - Premedication / Sedation: 0.02 - 0.05 mg/kg IV - Induction Dose: 0.1 - 0.3 mg/kg IV (depending on context) - Onset slower than propofol / thiopentone - Recovery prolonged with larger doses CVS / Respiratory Effects: - Mild fall in SVR/BP - Respiratory depression and apnea, especially with opioids or other depressants Advantages: - Amnesia - Anxiolysis - Useful as co-induction agent → reduces dose of other induction drugs Limitations: - Slower onset - Less reliable as sole rapid induction agent - Prolonged psychomotor impairment Midazolam vs Propofol vs Thiopentone: - PARAMETER: - Amnesia: Midazolam +++, Propofol ++, Thiopentone + - Onset (IV): Midazolam Slower, Propofol Very rapid, Thiopentone Rapid - Recovery: Midazolam Prolonged, Propofol Rapid, Thiopentone Intermediate - Respiratory Depression: Midazolam Mild → Moderate, Propofol Marked, Thiopentone Marked Reversal: - Flumazenil: Competitive benzodiazepine antagonist. Initial 0.2 mg IV → Repeat titration in small doses (0.1 mg) up to response. Exam Pearl: - Midazolam is better viewed as a co-induction/sedative drug than a classic rapid IV induction agent. Diazipam (Older): - Venous irritation / thrombophlebitis due to solvent (propylene glycol) - Prolonged action - Irritation / Phlebitis Lorazepam (Older): - Slower onset - Long duration - Not routine for IV induction Image 3: INTRODUCTORY SUMMARY - Intravenous induction agents are drugs used to produce rapid hypnosis/unconsciousness for induction of general anaesthesia. - Choice depends on hemodynamics, airway, intracranial status, comorbidities, and procedure. KEY THEMES - Onset - Redistribution - Context-sensitive recovery - CVS/RS/CNS effects - Dose - Advantages - Adverse effects - Contraindications INDEX - UPCOMING PAGES - Basics, definition, ideal properties, classification - Thiopentone & Methohexital - Propofol - Etomidate - Ketamine - Benzodiazepines in induction - Comparative tables & clinical selection - Viva pearls, mnemonics & references Image 4: Section heading: - Thiopentone Sodium: - Induction dose: 3-5 mg/kg IV (lower dose in elderly/hypovolemia) - Onset: 20-30 sec - Unconsciousness: ~1 arm-brain circulation time - Duration: 5-10 min (due to redistribution) - Highly lipid soluble - Alkaline solution, pH around 10-11; commonly 2.5% solution Section heading: Mechanism of Action - Positive allosteric modulation of GABA-A receptor → ↑ duration of Cl- channel opening → CNS depression - At higher doses, can directly activate GABA-A receptor (GABA-mimetic) → profound CNS depression Section heading: CVS Effects - Dose-dependent venodilation and myocardial depression → hypotension; compensatory / reflex tachycardia may occur Section heading: Respiratory Effects - Respiratory depression, apnea, blunted ventilatory response to CO2; may precipitate laryngospasm if airway stimulation occurs in light anesthesia Section heading: CNS Effects - ↓ CMRO2, ↓ CBF, ↓ ICP, ↓ IOP; cerebral protective effect in some settings; anticonvulsant Section heading: Other Effects - No analgesia Section heading: Adverse Effects / Complications - Extravasation → tissue injury, sloughing, necrosis - Intra-arterial injection → severe pain, vasospasm, ischemia, possible gangrene - Histamine release – uncommon but possible - Hiccups, coughing - Porphyria risk Section heading: Contraindication - Acute intermittent porphyria / porphyrias Section heading: Uses - Routine induction (historically, still used) - Neuroanesthesia - Refractory status epilepticus / barbiturate coma (concept note) Section heading: Methohexital - Induction dose: 1-1.5 mg/kg IV - Ultra-short acting; faster recovery - More excitatory phenomena and involuntary movements - Lowers seizure threshold / proconvulsant tendency - Useful for ECT Section heading: Comparison: Thiopentone vs Methohexital - Feature: - CNS depression: Profound (Thiopentone), Profound (similar) (Methohexital) - Seizure effect: Anticonvulsant (Thiopentone), Proconvulsant tendency (Methohexital) - Recovery: Slightly slower (redistribution) (Thiopentone), Faster recovery (very short acting) (Methohexital) - Use in ECT: Less commonly used (Thiopentone), Preferred agent for ECT (Methohexital) Image 5: FEATURE: - Induction dose: - Thiopentone: 3-5 mg/kg IV - Propofol: 1.5-2.5 mg/kg IV - Etomidate: 0.2-0.3 mg/kg IV - Ketamine: 1-2 mg/kg IV - Midazolam: 0.15-0.3 mg/kg IV - Onset: - Thiopentone: 30-60 sec - Propofol: 20-40 sec - Etomidate: 30-60 sec - Ketamine: 30-60 sec - Midazolam: 1-2 min - Duration after bolus: - Thiopentone: 5-10 min - Propofol: 3-8 min - Etomidate: 5-10 min - Ketamine: 10-20 min - Midazolam: 1-3 min - Analgesia: - Thiopentone: No - Propofol: No - Etomidate: No - Ketamine: Yes - Midazolam: No - Hemodynamic effect: - Thiopentone: ↓ BP (vasodilation myocardial depression) - Propofol: ↓ BP (dose dependent) - Etomidate: Minimal change (hemodynamically stable) - Ketamine: ↑ BP, ↑ HR (sympathomimetic) - Midazolam: ↓ BP (mild) ↓ SVR - Respiratory depression: - Thiopentone: Marked - Propofol: Marked - Etomidate: Mild - Moderate - Ketamine: Minimal - Midazolam: Moderate - Effect on ICP/CBF/CMRO2: - Thiopentone: ↓ ICP, ↓ CBF, ↓ CMRO2 - Propofol: ↓ ICP, ↓ CBF, ↓ CMRO2 - Etomidate: Neutral or slight ↓ ICP (well ventilated) - Ketamine: ↑ CBF, ↑ ICP, ↑ CMRO2 - Midazolam: ↓ CMRO2, minimal ICP ↓ - Bronchodilation: - Thiopentone: No - Propofol: No - Etomidate: No - Ketamine: Yes (marked) - Midazolam: No - PONV profile: - Thiopentone: High - Propofol: Low - Etomidate: Moderate - Ketamine: High - Midazolam: Moderate - Injection pain: - Thiopentone: Mild - Propofol: Marked - Etomidate: Minimal - Ketamine: Minimal - Midazolam: Minimal - Special advantage: - Thiopentone: ↓ ICP effect - Propofol: Rapid recovery Anti-emetic - Etomidate: Hemodynamic stability - Ketamine: Analgesia + Bronchodilation BP support - Midazolam: Amnesia Co-induction - Important adverse effect / key caution: - Thiopentone: Hypotension, apnea, Porphyria - contraindicated - Propofol: Hypotension, apnea, Pain on injection - Etomidate: Adrenal suppression (myoclonus rare) Avoid prolonged infusions - Ketamine: Emergence reactions, Hypersalivation, ↑ ICP (avoid in ↑ ICP states) - Midazolam: Respiratory depression, Hypotension (IV), Prolonged sedation CLINICAL SELECTION - SCENARIO BASED: - Hemodynamic instability / poor cardiac reserve → Etomidate (or Ketamine depending physiology) - Hypovolemia / trauma / severe asthma → Ketamine - Neurosurgery / raised ICP → Propofol, Thiopentone, or Etomidate (with controlled ventilation) - Day-care / high PONV risk → Propofol - ECT (Electroconvulsive therapy) → Methohexital - Seizure suppression / status epilepticus → Thiopentone or Propofol - Porphyria → Avoid barbiturates (Thiopentone, Methohexital) - Need analgesic induction → Ketamine - Septic patient with adrenal concern → Caution with Etomidate MEMORY AID: - Propofol = best recovery & antiemesis - Etomidate = best hemodynamic stability - Ketamine = analgesia + bronchodilation + BP support - Thiopentone = ↓ ICP, porphyria contraindication - Midazolam = amnesia / co-induction Image 6: Class: - phencyclidine derivative Mechanism: - moncompetitive NMDA receptor antagonist; also interacts with opioid, monoaminergic, and voltage-gated channels - Produces dissociative anesthesia DOSING: - Induction dose: 1-2 mg/kg IV - IM: 4-6 mg/kg - Onset (IV): 30-60 sec - Duration: ~10-15 min after IV bolus DISTINCT PROPERTIES: - Hypnosis + Profound analgesia + Amnesia - Cataleptic appear