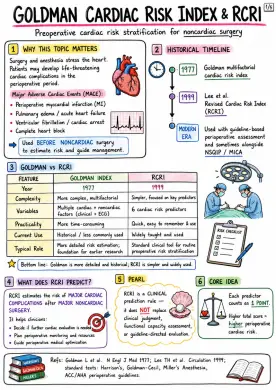
Goldman Cardiac Risk Index & RCRI
RCRI estimates the risk of MAJOR CARDIAC COMPLICATIONS after MAJOR NONCARDIAC SURGERY. Image 1: Why This Topic Matters: - Surgery and anesthesia stress the heart. - Patients may develop life-threatening cardiac complications in the perioperative period. - Major Adverse Cardiac Events (MACE): - Perioperative myocardial infarction (MI) - Pulmonary edema / acute heart failure - Ventricular fibrillation / cardiac arrest - Complete heart block - Used BEFORE NONCARDIAC surgery to estimate risk and guide management. Historical Timeline: - 1977: Goldman multifactorial cardiac risk index - 1999: Lee et al. Revised Cardiac Risk Index (RCRI) Goldman vs RCRI: - FEATURE - Year - Goldman Index: 1977 - RCRI: 1999 - Complexity - Goldman Index: More complex, multifactorial - RCRI: Simpler, focused on key predictors - Variables - Goldman Index: Multiple cardiac + noncardiac factors (clinical + ECG) - RCRI: 6 cardiac risk predictors - Practicality - Goldman Index: More time-consuming - RCRI: Quick, easy to remember & use - Current Use - Goldman Index: Historical / less commonly used - RCRI: Widely taught and used - Typical Role - Goldman Index: More detailed risk estimation; foundation for earlier research - RCRI: Standard clinical tool for routine preoperative risk stratification What does RCRI predict? - RCRI estimates the risk of MAJOR CARDIAC COMPLICATIONS after MAJOR NONCARDIAC SURGERY. - It helps clinicians: - Decide if further cardiac evaluation is needed - Plan perioperative monitoring and resources - Guide perioperative medical optimization Pearl: - RCRI is a CLINICAL prediction rule – it does NOT replace clinical judgment, functional capacity assessment, or guideline-directed evaluation. Core Idea: - Each predictor counts as 1 POINT. - Higher total score = higher perioperative cardiac risk. Modern Era: - Used with guideline-based perioperative assessment and sometimes alongside NSQIP / MICA. Image 2: Concept: - Goldman created a weighted multifactorial index for predicting serious perioperative cardiac complications in noncardiac surgery. Predictors & Points: - S3 gallop or elevated JVP: 11 points - Myocardial infarction within previous 6 months: 10 points - >5 premature ventricular contractions per minute preoperatively: 7 points - Rhythm other than sinus or presence of PACs on preoperative ECG: 7 points - Age >70 years: 5 points - Emergency operation: 4 points - Intraperitoneal, intrathoracic, or aortic surgery: 3 points - Important aortic stenosis: 3 points - Poor general medical condition: 3 points Poor General Medical Condition Includes: - Hypoxemia - Significant electrolyte or acid-base disturbance - Renal dysfunction - Hepatic dysfunction - Bedridden / poor systemic status Risk Classes: - Class I: 0-5 points - Class II: 6-12 points - Class III: 13-25 points - Class IV: ≥26 points Strengths / Weaknesses: Strengths: - Historically seminal - Introduced structured perioperative cardiac risk assessment Weaknesses: - Cumbersome, weighted variables - Depends partly on ECG findings - Less practical now - Largely replaced by simpler models Take-Home Pearl: - Goldman index is high-yield for exams and history of perioperative medicine, but RCRI is more commonly used in routine practice. - Approx historical life-threatening cardiac complication rate in derivation cohort rose markedly across classes (~1%, 7%, 14%, 78%). Image 3: How Scoring Works: - Each variable = 1 point - Total score = 0–6 Original Endpoint: - Predicts risk of MAJOR CARDIAC COMPLICATIONS: - Myocardial infarction (MI) - Pulmonary edema - Ventricular fibrillation or primary cardiac arrest - Complete heart block 6 Predictors - 1 Point Each: - High-risk surgery: intraperitoneal, intrathoracic, or suprainguinal vascular surgery - History of ischemic heart disease: prior MI, positive stress test, typical angina/current ischemic chest pain, nitrate therapy, or pathologic Q waves - History of congestive heart failure: prior HF/pulmonary edema/PND, bilateral rales or S3, or pulmonary vascular congestion - History of cerebrovascular disease: prior stroke or TIA - Diabetes mellitus requiring insulin therapy - Preoperative serum creatinine >2.0 mg/dL (177 micromol/L) Memory Line: - High-risk surgery + IHD + CHF + CVA + insulin DM + Cr >2 Clinical Pearl: - RCRI is simple and fast, but it estimates risk — it does not itself dictate stress testing or cancellation of surgery Compared to Goldman: - Unlike Goldman, RCRI uses six binary variables with equal weight. Image 4: RISK CLASSES: - Original Lee et al. rates for major cardiac complications - RCRI SCORE (# OF PREDICTORS) - 0 PREDICTORS: CLASS I, 0.4% APPROX. RISK OF MAJOR CARDIAC COMPLICATIONS - 1 PREDICTOR: CLASS II, 0.9% APPROX. RISK OF MAJOR CARDIAC COMPLICATIONS - 2 PREDICTORS: CLASS III, 6.6% APPROX. RISK OF MAJOR CARDIAC COMPLICATIONS - ≥3 PREDICTORS: CLASS IV, 11.0% APPROX. RISK OF MAJOR CARDIAC COMPLICATIONS - Major cardiac complication = MI, pulmonary edema, VF/cardiac arrest, or complete heart block HOW TO READ IT CLINICALLY: - 0 = low perioperative cardiac risk - 1 = mildly increased risk - 2 = clearly elevated risk - ≥3 = high risk; consider more intensive perioperative planning STRENGTHS: - Simple - Bedside - Reproducible - Externally validated - High-yield teaching tool LIMITATIONS: - Calibration varies in modern populations - May underestimate risk in some vascular surgery patients - Does not include frailty, age, functional capacity/METs, biomarkers, active valvular disease, urgency, or intraoperative factors - Should not be used as the only decision-maker OTHER TOOLS: - Other tools such as NSQIP MICA / ACS NSQIP may offer procedure-specific individualized estimates in some settings. Image 5: Practical Stepwise Approach: - Determine urgency of surgery (emergent / urgent / elective). - Look for active unstable cardiac conditions: - Acute coronary syndrome / unstable angina - Decompensated heart failure - Significant arrhythmia - Severe valvular disease - Estimate surgical risk and calculate RCRI. - Assess functional capacity (METs): if ≥4 METs and no unstable features, often proceed without further testing. - If elevated risk and poor / unknown functional capacity, consider biomarkers and/or noninvasive testing only if results will change management. - Optimize perioperative plan: monitoring, medications, postoperative surveillance. Medication Pearls: - Continue chronic beta-blockers; do not start high-dose beta-blocker on day of surgery. - Continue statins, especially for vascular surgery patients. - Antiplatelet and anticoagulant decisions are individualized. - Consider postoperative troponin surveillance in selected high-risk patients. Important Pitfalls: - Not designed for cardiac surgery. - Do not use RCRI alone to cancel surgery. - Combine with surgical factors, history, exam, ECG, functional capacity, and guidelines. - Absolute risk may differ from the original 1999 cohort. RCRI vs Other Tools: - RCRI: simplest bedside score. - NSQIP MICA/ACS NSQIP: more individualized procedure-specific risk estimation.